patient information - Rolle + Rolle
Hauptmenü:
patient information
products > eraser surgical laser
Information about surgery for lung metastases
This page is designed to inform you comprehensively of the latest status of treatment options available and, in particular of the newly developed laser technology with the surgical treatment of lung metastases. Furthermore, you will learn the key requirements that are necessary for laser surgery and who can be considered for such a procedure as a patient.
350,000 new cancer patients in Germany every year
Today, cancers occur in at least 20 per cent of our population, making them the second most frequent disease directly after cardiovascular diseases. For Germany, this means in figures that about 350,000 fall ill with cancer every year. Of this figure, every third patient will have to accept that lung metastases will develop in the course of their cancer disease. Unfortunately, the opinion that an end stage is reached when these lung metastases occur is still very common. The belief is that nothing can be done for the patient apart from possibly chemotherapy. Little is known that the surgical removal of lung metastases has been a key topic in the special area of thoracic surgery for a good 20 years. In addition, there is today a technical development in laser technology that allows including a larger number of patients in the surgical treatment of removing far larger numbers of metastases in a way that is gentle on the tissue.
What kind of a surgical method is this?
To begin with, the surgery described below is a service that is covered by all health insurance companies that is nowadays offered in many thoracic surgery clinics. Contrary to the far more frequently used bracket seam resection, the laser resection, however, is far more gentle on the patient, as less healthy tissue needs to be removed, a far higher number of metastases can be removed and the procedures can therefore also be repeated several times if new metastases occur. The basic device consists of a patented diode laser that can radiate a new wave length (1318 nanometres) in previously unattainable strength and quality. The laser radiation has only in this wave length properties that are particularly well-suited to performing surgery on the lung tissue, as the lung differs strongly from other organs. This affects, in addition to the strong blood circulation of the lung, the air content and the fineness of the tissue in particular. In order to enter the chest, bendable quartz fibres especially optimsed for this wave length are connected to the laser device, which act as a laser scalpel. When cutting into the lung tissue with traditional instruments, strong bleeds occur quickly with a simultaneous air release, which make penetration into the depth of the lung impossible. With the laser device stated, the thoracic surgeon, however, can simultaneously cut, clot blud and prevent the air release by additionally shrinking the tissue. As such, it is possible to reach all lung areas and cut out metastases that are located in the middle of a lobe of the lung without having to remove the entire lobe. A far higher number of metastases can also be removed than in the past (highest number of metastases removed amounts to about 300).
How is the surgery carried out?
To be able to remove the metastases, the chest is opened by making a small lateral cut (for women in the breast fold). Subsequently, the half of the lung that is affected is disconnected from the air supply, which results in it shrinking to about one third of its ventilated size. In this condition, it can be felt with precision by an experience thoracic surgeion for metastases up to a size of one millimetre. This means that the examination during surgery is even more precise than the examination technique common today with a spiral computer tomogram that records metastases up to a size of three to five millimetres. The metastases there by localised (or tumours of another type) are then circumvented with the laser ray at a small safety distance and cut out of the healthy lung tissue. As this is a so-called photothermal removal of the metastases, this means that during the cutting out, temperatures are reached of up to 300 degrees celsius, the safety distance and therefore the tissue loss can be kept small, because at such high temperatures tumour cell spreading can be virtually ruled out. Nevertheless, all materials and metastases removed can be examined by the pahtologist microscopically and in an immune histochemicall manner. In such a way, metastasis for metastasis is removed from the relevant segments of a lobe of the lung and - where required - further lobe for lobe (three lobes on the right, two lobes on the left) are cut out and the function of the remaining lobe remains preserved. After removing the metastases, lymph nodes are then removed from all key areas, as their examination provides further information. If both lungs are affected with metastases for a patient, the more strongly affected side is started on. Once the side subjected to surgery has then recovered after about four weeks, the second lung is subjected to surgery in the same way. This procedure is particularly gentle, avoids complications and maintains a high level of quality of life for the patient also in the event of a large number of metastases. Finally, this tissue-spanning and gentle laser surgical method opens up the possibility of a second, third or even fourth course of treatment, if metastases again occur in the further process.
For which patients is the surgery possible?
As a rule, you need to be in a good general condition and be of strength and have a sufficient lung function (be able to climb about two storeys without interruption because of paraxysmal dyspnea). Metastasis can be removed from all kinds of primary tumours, for instance: colorectal cancer, kidney and bladder cancer, breast cancer, lung cancer, bone cancer, malign melanome, and so on. However, only the lungs should be affected by metastases and no other organ. If, for instance, thre are also liver metastases or brain metastases, the surgery of the lung metastases can only be carried out if these other metastases have been fully removed surgically (the laser technology can also be used for this) or brought to a full regression by another treatment. Furthermore, the primary tumour (for instance colorectal cancer, breast cancer, lung cancer and so on) also needs to have been fully removed or brought to a full regression through a special treatment. Patients with a larger number of lung metastases and lung metastases on both sides can also be considered for the treatment. However, the final assessment on the basis of a current computer tomograph is carried out by the attending thoracic surgeon. Furthermore, patients whose lung metastases were already detected with the primary tumour can also be considered, as well as patients for which metastases are again growing in the lung following removal of lung metastases. In these cases the final assessment is also carried out on the basis of a current computer tomograph by the thoracic surgeon.
What preliminary examinations are necessary?
In addition to the generally necessary examinations that are needed for surgery, a lung function examination should objectify your performance.
To rule out any impact on other organs:
- Ultrasound of the liver,
- or computer tomograph of the abdomen
Bone or sceleton scintigram In order to assess the primary tumour and any local residue:
- Relevant current examination of the primary tumour region, including any possible mirroring (for instance coloscopy)
- or, for instance, magnetic resonance tomography (MRT) in bone tumours.
If you are looking for a clinic with this technology or have other questions, please do not hesitate to contact us. You can contact us on the number stated under the Contact category.
Are you looking for a hospital that offers that kind of treatment?
Please contact us and we are going to help you to find a hospital offering that special laser treatment.
Please contact us and we are going to help you to find a hospital offering that special laser treatment.
The movie is highlighting the differen between the eraser resection and a stapler resection: the us of a stapler causes unnecessary loss of healthy tissue. Central and/ or multiple metastases can't be resected using a stapler.
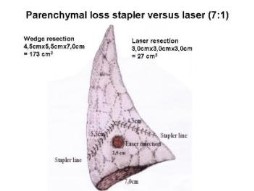
Comparison of loss of tissue laser versus stapler. Laser: 27 cm³, stapler: 127 cm³.
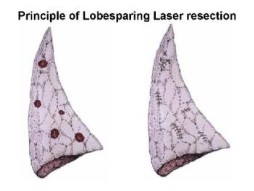
In case of multiple metastases, the conventional procedure leads to the loss of a whole lung lobe, which means the loss of about 20% of the whole lung. When the erasr is used, every single metastasis can be resected and almost all healthy lung tissue can be safed.